
RVNAhealth registered dietitian and nutrition educator, Ava Safir, JD, MS, RDN, shares her experience with the Intermittent Fasting diet.Continue reading

![]() Give to RVNAhealth on Fairfield County’s Giving Day, February 25, and become our partner in fighting COVID-19. Your support will sustain our vaccination clinics and protect our communities.
Give to RVNAhealth on Fairfield County’s Giving Day, February 25, and become our partner in fighting COVID-19. Your support will sustain our vaccination clinics and protect our communities.
Learn more at fcgives.org ››

Did you know that one in three U.S. adults has high blood pressure? By 2030, it is expected that over 41 percent of U.S. adults will have this condition. The normal blood pressure for adults age 20 or over is no higher than 120/80 mm Hg (millimeters of mercury).
The first number in your blood pressure reading is always larger and refers to systolic BP (the pressure in the arteries when the heart beats). The second number in the reading is always smaller and refers to diastolic BP, the pressure in the arteries when the heart rests between beats and refills with blood.
RVNAhealth offers blood pressure screenings throughout each month. View our Community Events Calendar for dates, times and locations.
The infographic below from the American Heart Association is a handy source for understanding your blood pressure and recommendations for ensure that you get a proper reading.
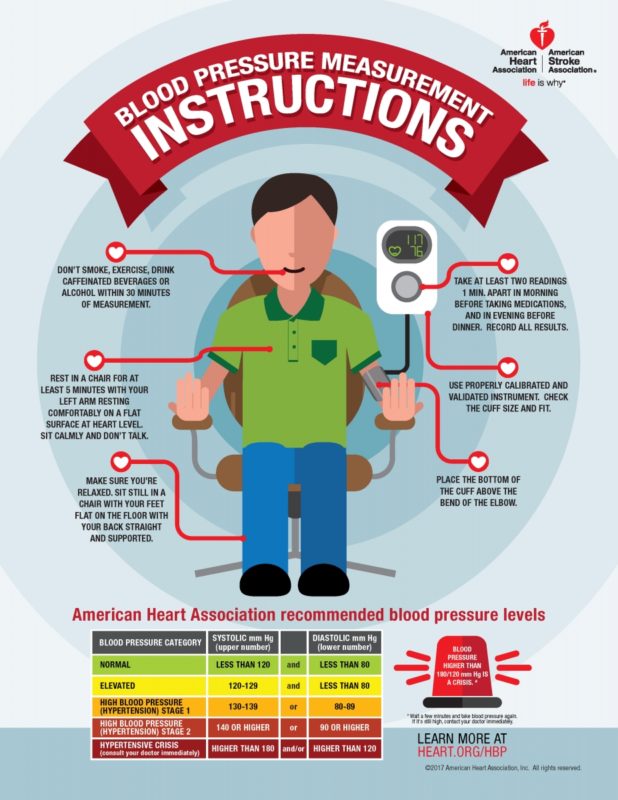
Recommendations include:







Above: Tammy Strom, MA-MTBC, plays her guitar at RVNAhealth’s headquarters on Governor Street in Ridgefield.
When Tammy Strom, MA-MTBC, visits RVNAhealth hospice patients, she’s equipped with a distinctive set of clinical tools. A guitar. Piles and piles of sheet music and songbooks. And a variety of handheld musical instruments (think tambourines, shakers, bells and other fun accessories).
As our hospice music therapist, Tammy also brings healthy doses of compassion and positivity, alongside a dedication to helping patients experience the best possible quality of life in their final months, weeks and days.
“Many people have the misconception that working with hospice patients is somber,” she says. “But as a music therapist I get to see, and be a part of, a lot of life and creativity.”
When hearing the term “music therapy,” you might think of listening to music performed by someone else. Or the opportunity for a patient and perhaps the family to play, sing or even write songs. The reality is that it depends – on what goals are appropriate for the patient and family.
Tammy shares how, in the case of a patient who had difficulty speaking, the simple act of slowing down a beloved song so she could sing brought “great joy” to both the patient and her family.
“If you’re with them for several months, as their condition progresses, it might be more about soothing with music that carries meaning,” she adds. She recalls this being the situation with a patient who was no longer alert, but the husband requested their wedding song from long ago.
“Musical interventions aren’t about being note-perfect, and it isn’t about teaching music,” explains Tammy. “It’s focused on providing comfort and memories. The goal might be to alleviate isolation; help a family connect with a patient who is unable to speak due to dementia; or distract from the patient’s physical discomfort or soothe the emotional pain the patient and family are experiencing.”
Music therapy can also be used as a restorative therapy in the bereavement process, especially with children mourning a loss.
Hospice music therapy is administered by a credentialed professional who has completed an approved music therapy program and passed a national exam offered by the Certification Board for Music Therapists. In addition to being board certified in music therapy, Tammy holds a master’s degree in expressive therapies with a concentration in music therapy and mental health counseling. A lifelong musician, she has sung with the Ridgefield Chorale for two decades, and has performed with Troupers Light Chorale in the past.
“Music stimulates many parts of the brain – from auditory to motor to emotional – and it is often one of the last memories to remain intact,” she stresses. “Many studies have found that music therapy positively affects patients’ quality of life by addressing their spectrum of needs: Physical, psychological, emotional, spiritual, social and family support.”
Also, as she is fond of saying, in the words of Hans Christian Andersen: “Where words fail, music speaks.”
Read More Hospice & Palliative Care Month Articles
Hospice is for Living
How Spiritual Care Providers Help Hospice Patients and Their Families

The following essay was written in 2019 by Keri Linardi, RN, BSN, PHN, CHPCA, Chief Clinical Officer of RVNAhealth. Keri is, has been, and always will be a hospice nurse — in addition to the other roles she assumes. Hospice care is part of Keri’s being, part of her heart and the key to how she approaches her life.
This month, November, is Hospice and Palliative Care Month. In her words below, Keri shares her perspective on how hospice has impacted her and her children’s lives, and what we can do this month to plan for our own futures.
Children raised in the home of a hospice nurse, like me, live in a world where death and dying, and ending suffering are talked about freely. During my years of night shifts, my young children would ask over breakfast, when I returned home, how many people had died last night, and we would talk about the beautiful deaths I was privileged to bear witness to.

Some of the stories were funny, like the husband who called me when his wife had passed in the middle of the night, only for me to discover, when I touched her and she sat up, that she was still very much with us. To the ones that touched too close to home, like the children near to my own children’s ages, so that when I went to the car after leaving their homes, I sobbed uncontrollably for what seemed like forever, for a life lost too soon and for families who would have holes in their hearts that would never be repaired, just healed with memories over time.
We are a country that has plans for everything from birth, to vacations, yet we don’t plan for our own mortality. Dying sneaks up on families and throws them into decision making in moments of crisis — a time when decisions should not be made!
Being a child of a hospice nurse is a double-edged sword: we never hang up the phone without saying ‘I love you;’ I have never sweated the small stuff with them, you want magenta hair?, it’s your head, go for it! The flip side is we talk about mortality – particularly my own — over family dinners. This bothers my children a little, now ages 22, 19 and 13, but I need them to understand in simple terms what my wishes are if anything were to happen to me, and I need them to know that they will not be making decisions but simply honoring my wishes, decisions I have already made. They also fully understand that dying is a natural part of living, the circle of life.
In times of crisis, these ‘already-had conversations’ can be the greatest gift you give your loved ones, the gift of them knowing exactly what you would want to do. The gift of them knowing that they are not making the decisions for you when you aren’t able, they are honoring you one last time by following your wishes.
As a hospice nurse, who has seen families grappling with decisions at critical times, this is a gift I would like everyone to give their loved ones.
But we aren’t there yet.
In this country we have disparities in care that interfere with individuals’ abilities to access hospice care when it is needed most. A study from Duke University in 2018 outlines that African Americans, 13.4% of the population, make up only 8% of hospice patients in America and are more likely to suffer from untreated pain; Hispanic patients, who represent 18.3% of the US population, make up 7% of hospice patients nationally. There are cultural barriers that interfere with their access to hospice care.
We need to work together to change this and to provide culturally competent care at the right time – and we need to dispel the many myths around hospice care.
The hospice Medicare benefit is a six-month – approximately 180 day — benefit of care that provides support from a whole team of professionals who wrap themselves around the patient and family to help them through one of the most challenging times of their lives. In my 26 years of nursing, I have never had a family tell me they came on to hospice too soon. I have had many families tell me, “If I had only known what hospice was, I would have called sooner.”
Despite the 180-day benefit, the national average length of stay for hospice care in the country right now is 21.5 days; for the state of Connecticut it is 14 days. This means that as a state, we aren’t doing a very good job at acknowledging life-limiting conditions head on — in a direct, kind, caring manner. We are introducing hospice care too late in the process and we are denying patients and their families care, comfort and treasured time when they need it the most.
Often when hospice is offered as an option, it is presented in negative terms – “There isn’t anything more to do;” Do not resuscitate,” — when in fact there is a lot of living and a lot of joy that occurs in hospice.
When life-limiting conditions occur, we in hospice care talk about allowing natural deaths, managing symptoms, and living every day to its fullest. Imagine if you knew you only had six months left to live — would you do anything differently?
Hospice care has filled my cup these past 20 plus years in nursing. I am appreciative and grateful to the patients whose hands I have held; to those whose windows I have gazed out of, together enjoying their favorite hydrangeas; the families whose strength and grace I have marveled at as they cared for their loved ones through to the end. The kindness they have shown me as guests in their home.
I am amazed daily at the wonderful team of hospice people at RVNAhealth that come to work and give of themselves every day for our community and patients and families. And to you, our RVNAhealth hospice families. I am in awe of you and thank you for allowing us to be guests in your home and into your lives during this very private time. I honor you during this special month.
In closing, I would encourage anyone who has not yet started their Advanced Care Planning conversations to use this November as your springboard to make the move! Start the conversation about Advanced Care Planning, visit our hospice and palliative care team at RVNAhealth. Let us help you start the conversation during non-crisis times. We have educational handouts to guide you, as well as team members to speak with. Nobody has ever regretted the decision to plan in advance. On the contrary. It’s a gift to yourselves and your loved ones.
To learn more, contact 203-438-5555 or visit our Hospice Services page.
Read More Hospice & Palliative Care Month Articles
Hospice Music Therapy Provides Comfort and Memories
How Spiritual Care Providers Help Hospice Patients and Their Families